Introduction
Active middle ear implants are an alternative treatment option for various forms of hearing loss. The classic indication for the use of the Vibrant Soundbridge (VSB, MED-EL, Innsbruck, Austria) is sensorineural hearing loss, in which case the floating mass transducer (FMT) is crimped to the long process of the incus with a titanium clip.1) When used to treat mixed hearing loss, in which the middle ear is diseased and the inner ear requires amplified auditory input, the FMT can also be used together with various titanium couplers to ease the attachment of the FMT to the ossicles of the middle ear or to the oval or round window, thereby stimulating the inner ear. Furthermore, the FMT in conjunction with a coupling element can be used not only as an active prosthesis but also works as a passive prosthesis without activation of the speech processor.2)
In 2006, a Bell partial prosthesis in combination with an FMT was tested in three temporal bones.3) Although the results of laser Doppler interferometry were encouraging, the lateral attachment of the prosthetic shaft to the FMT runs the risk of prosthesis tilting; thus, this Bell vibroplasty technique has not been widely performed. In 2011, the concept was improved by the development of Clip-PORP-Vibroplasty.4) The coupler combines a titanium clip holder for the FMT with the classic mechanism that involves fitting the clip onto the stapes head in a standardized way, as with passive partial clip prostheses.5) This linear integration of the FMT in a titanium column with additional fastening by a clip mechanism adds potential stability and long-term safety to the construction. This coupling element is also available with a bell-shaped attachment (Vibroplasty-Bell-Coupler) to the stapes head.
We report herein a case involving a patient with VSB who underwent stapes clip coupler placement at the stapes head.
Case Report
A 65-year-old man with postlingual-onset hearing loss was diagnosed with bilateral mixed severe hearing loss due to chronic otitis media. He had used conventional hearing aids in both ears for more than 3 years, but he no longer used his right hearing aid because of discomfort. He experienced difficulty in using the telephone.
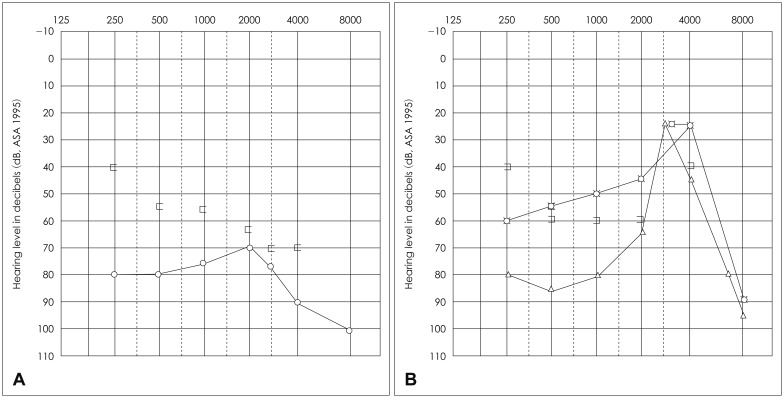
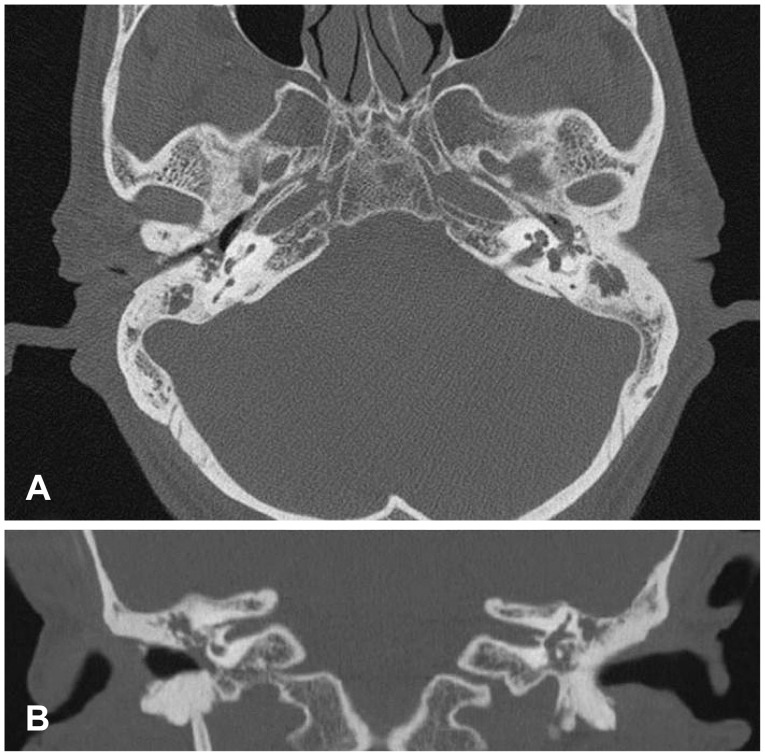
Otoscopic examination revealed sclerotic tympanic membranes without perforation or effusion. A pure tone audiogram revealed bilateral symmetrical mixed hearing loss with an average air conduction threshold of 78 dB in the right ear and 69 dB in the left (Fig. 1). Speech discrimination scores were 62% for the right ear at 104 dB most comfortable listening (MCL) and 88% for the left ear at 98 dB MCL without hearing aids. He used the left-sided conventional hearing aid only. In the left ear, aided pure-tone audiometry showed 50 dB and aided speech audiometry showed 86% at 70 dB MCL (Fig. 1B). Sclerotic changes in the mastoid cavity, a normal ossicular chain, and soft tissue filling the middle ear cavities were noted on preoperative temporal bone CT scans. The patient was suspected to have bilateral chronic otitis media (Fig. 2).
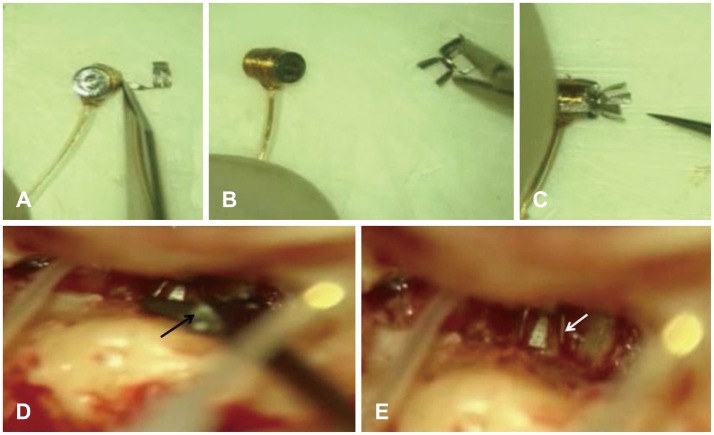
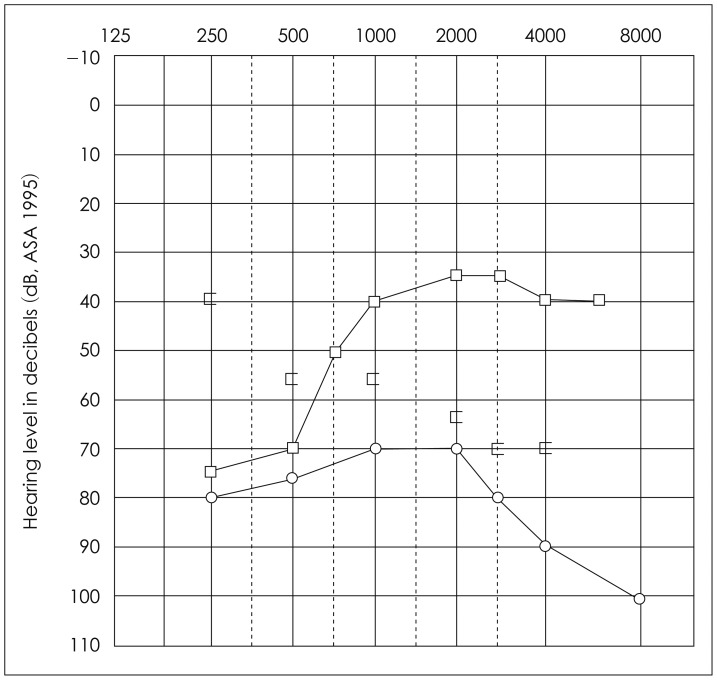
We planned a right mastoidectomy to control the inflammation, and placement of a right middle ear implant to improve hearing. During the operation, we first performed a simple mastoidectomy to remove sclerotic mastoid air cells and granulation, then widely opened the facial recess. Although soft tissue around the ossicular chain was removed, incudostapedial joint fixation noted. The incudostapedial joint was separated to confirm stapes mobility. Because stapes mobility was intact, incus was then removed and the VSB internal device (MED-EL; Innsbruck, Austria) was implanted. After cutting the attachment clip of the FMT with surgical knife (Fig. 3A), the FMT was inserted into a clip coupler (Fig. 3B). The coalescent clip coupler-FMT complex (Fig. 3C) was connected to the intact head of the stapes (Fig. 3D). Fixation between the clip coupler-FMT complex and stapes head was stabilized by clipping (Fig. 3E). Harvested conchal cartilage was inserted between the FMT and tympanic membrane to prevent protrusion of the clip coupler-FMT complex. The patient was discharged on the second day postoperatively without complications. Six months after the operation, the patient showed a decreased air-bone gap on mid frequencies even without the speech processor (>5 dB decrease on 0.5 & 1.0 kHz). Additionally, on activation of the speech processor, vibroplasty can actively improve mid- and high-tone frequency hearing and patients showed more efficient sound transmission (Fig. 4).
The Abbreviated Profile of Hearing Aid Benefit (APHAB) questionnaire, which assesses the performance of, and satisfaction with, hearing aids, was administered before and after the operation. The APHAB score showed marked improvement from 76.0 points preoperatively to 12.8 points postoperatively (ease of communication, 0; reverberation, 17; background noise, 17; aversiveness, 17).
Discussion
Originally, the VSB was designed for the treatment of sensorineural hearing loss in normal middle ears. With the clip holder, it can now also be used in pathologic middle ears with a stable and reliable attachment. Previous experiments have shown that inner ear stimulation is more effective than conventional hearing aids and passive middle ear implants in pathologic middle ear conditions.
The hearing outcome in our case was more satisfactory than those in previous reports of partial ossicular reconstruction prosthesis coupling on the stapes head. Efficient sound transmission was clinically confirmed according to the temporal bone experiments.3)
Our patient reported very comfortable hearing even without the use of a speech processor. Upon application of the speech processor, the patient exhibited a marked improvement in the hearing threshold and great comfort of use, which were shown by the results of the APHAB Questionnaire.6,7) These positive outcomes can be explained by involvement of both passive and active pathways. Use of the clip vibroplasty device alone can produce passive PORP effects by adjust the thickness of reinforcement cartilage. Additionally, on activation of the speech processor, vibroplasty can actively improve high-tone frequency hearing and speech discrimination without the occlusion effect.8,9)
Clip vibroplasty is recommended only after complete eradication of any infectious disease of the ear in patients with chronic otitis media, and the cable of the implant should be protected behind thick cartilage plates. Two step approaches for clip vibroplasty should be considered if any infectious condition is remained.
Because of the improvement in hearing and ease of handling, similar to the placement of a passive prosthesis, the indications for this power clip may make it a promising alternative for patients with conductive hearing loss who got poor results from passive middle ear implants (ossiculoplasty).